Home | About OC | Continuing Education | Course Schedule | Registration | Accommodations | About Dr. Chan | Study Club | Doctor Education | Patient Education | Vision | Research Group | Science | Orthodontics | Laboratory | Dr. Chan’s Articles | GNM Dentistry | Contact Us | Dr. Chan’s Blogs

Airway Obstruction: Primary Environmental Factors
Poor arch development, lack of tongue space, facial aesthetics, tooth long axis discrepancies, anterior crowding, and vertical deficiencies are growth and development outcomes of abnormal tongue habits, airway obstruction (breathing), muscle abnormalities, postural abnormalities and facial abnormalities. These are just some of the primary environmental factors that leads to skeletal and neuromuscular problems of any patient with multiple influences.

A comprehensive understanding of the early iatrogenesis of aberrant tongue function is available in the Garry’s monographs on “Early iatrogeneic orofacial muscle, skeletal, and TMJ dysfunction”. Placement of the tongue to maintain a compensatory airway due to nasal obstruction or placement of the tongue between the teeth for compensatory bracing of the mandible may also lead to unstable occlusion.
Science has shown that nasal airway obstruction is caused by hypertrophied tonsils and adenoids, inflamed turbinates, allergic and nonallergic rhinitis, vasomotor rhinitis, deviated septum and posterior choana stenosis. Harvold’s experiments demonstrated that the recruitment of orofacial muscles for respiration have a significant effect on muscle development which changes the morphology of the upper lip, the tongue, and orophayrngeal opening. It has been noted that lip and tongue changes are followed by remodeling of the alveolar process and changes in direction of tooth eruption that results in subsequent malocclusion.<1>
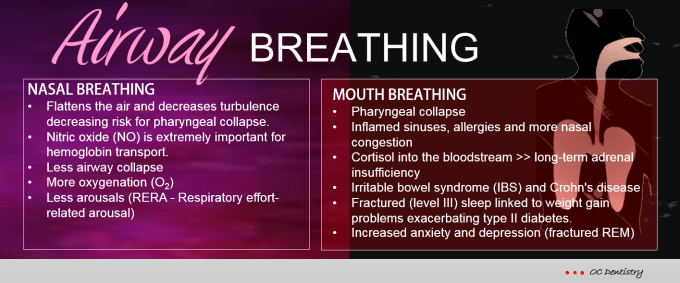
Nasal Breathing vs. Mouth Breathing

Development of Craniomandibular Dysfunctions Resulting from Upper Respiratory Allergies
- Food contactants and / or Inhalant allergies –> Release of Chemical mediators such as histamine, Kinins, Slow reacting Substances of Anaphylaxis (SRA), and Eosinophilic Chemotactic Factor (ECF)….thus leads to Allergic edema of the nasal and paranasal mucosa, i.e., allergic rhinitis. ——-> venous puddling with capillary stagnation, mouth breathing, lowering of oxygen saturation resulting in local tissue acidosis, acid/alkaline imbalance (decreased alkali reserves), interference with optimal growth and development, i.e., facial asymmetry —> lower resistance to injections hypertrophy of adenoid tissues, obstructive desyfunction of the eustachian tubes —> bruxism, malocclusion, craniomandibular dysfunctions (loss of vertical) along with a chain of other events and constellation of numerous issues (not stated here in this post) leading collapse of the maxillo-mandibular dental arches, high vault palates, reduced nasal airway/inadequate volume for tongue within the dental arches to th eventual poor tongue repose —–>Malocclusion —–> neuromuscular closed bite or open bite, crowding, crossbite, lateral and or posterior displacement of mandible —-> Craniomandibular Dysfunction.
__________________________
Related information on Upper Airway Compromise:
- The Legacy of James F. Garry, D.D.S. – “The Einstein of Dentistry” – A power point presentation
- James F. Garry, DDS – Pioneer in Upper Airway Compromise and Musculoskeletal Dysfunction
- Airway Obstruction: Environmental Influences
- “In Loving Memory of My Great Mentor and Dear Friend, Dr. James F. Garry.”
- Upper Airway Obstruction and Upper Airway Deformaties – Part 1
- Upper Airway Obstruction and Upper Airway Deformaties – Part 2
- Upper Airway Obstruction and Upper Airway Deformaties – Part 3
Reference:
- Harvold EP: Neuromuscular and morphological adaptations in experimentally induced oral respiration, In Naso-respiratory function and Craniofacial Growth. McNamara, JA., ed., Mono-9, Craniofacial Growth Series, Center for Human Growth and Development, Univ, Of Michigan, Ann Arbor, 1979, pp 49-164.
- K Sato, T Shirakawa, H Sakata and S Asanuma: Effectiveness of the analysis of craniofacial morphology and pharyngeal airway morphology in the treatment of children with obstructive sleep apnoea syndrome. Dentomaxillofacial Radiology (2012) 41, 411–416.
- Carole L. Marcus, M.B., et. al.: A Randomized Trial of Adenotonsillectomy for Childhood Sleep Apnea. N Engl J Med. 2013 June 20; 368(25): 2366–2376.
______________________
Read More: TMD Problems that Challenge Dentistry – Four Main Categories
- TMD: Cervical Dysfunction Problems
- TMD: Temporomandibular Joint Primary Problems
- TMD: Anterior Open Bite Tendency Problems
- Tongue Posture and Abnormal Swallowing Patterns Contributing to Hyper Muscle Activity and TMD
To Read More: Initial Treatment Protocol
![]()
9061 West Post Road, Las Vegas, Nevada 89148 United States Telephone: (702) 271-2950
![]()
Leader in Gneuromuscular and Neuromuscular Dentistry